Understanding Shoulder Impingement and Rotator Cuff Related Shoulder Pain: What Does the Research Actually Say?

Shoulder pain is one of the most common musculoskeletal problems seen in physiotherapy, particularly in people who train regularly, work in repetitive positions, or perform frequent overhead movements.
Terms like shoulder impingement, rotator cuff tendinopathy, and subacromial pain syndrome are often used interchangeably — sometimes creating more confusion than clarity. Modern research has gradually shifted the way clinicians understand these conditions, with increasing focus on load management, tendon health, and shoulder function rather than the idea of structures simply being “trapped” or “pinched.”
At Centre of Gravity Physiotherapy Farnborough, treatment for shoulder pain is guided by current evidence alongside detailed clinical assessment. Understanding what research actually tells us can help people make better decisions about recovery, exercise, and long-term management.
What Is Shoulder Impingement?
Traditionally, shoulder impingement was thought to occur when the rotator cuff tendons became compressed underneath the acromion — part of the shoulder blade — during overhead movement.
While compression can still contribute to symptoms in some people, modern research suggests the situation is often far more complex than simply “bone rubbing on tendon.”
Studies now show that many people without any shoulder pain at all have:
Rotator cuff tendon changes on scans
Reduced subacromial space
Tendon thickening or degeneration
Partial rotator cuff tears
At the same time, many people with significant shoulder pain show relatively minor findings on imaging.
This has led to a growing understanding that shoulder pain is influenced not only by tissue structure, but also by:
Tendon loading capacity
Strength and conditioning
Movement control
Repetitive overload
Recovery and adaptation
Sensitivity of surrounding tissues
As a result, the term Rotator Cuff Related Shoulder Pain (RCRSP) is now commonly used in research and physiotherapy practice.
The Role of the Rotator Cuff
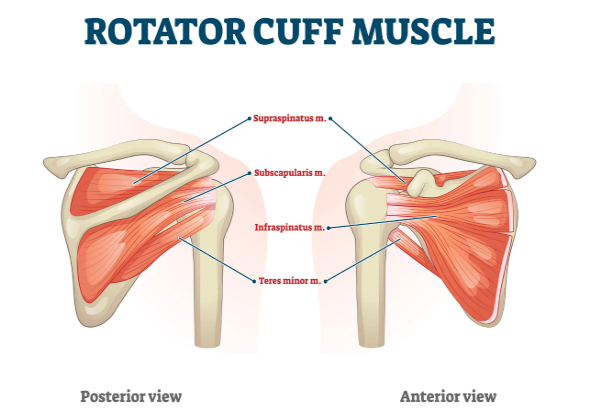
The rotator cuff consists of four muscles that help stabilise and control the shoulder joint during movement.
Supraspinatus
Helps lift the arm out to the side
Commonly involved in shoulder pain and tendinopathy
Infraspinatus
Helps rotate the arm outward (external rotation)
Important for shoulder stability during pulling and overhead movements
Teres Minor
Assists with external rotation of the shoulder
Works closely with the infraspinatus
Subscapularis
Helps rotate the arm inward (internal rotation)
Provides significant front-of-shoulder stability
These muscles play a major role in:
Overhead movement
Gym and strength training
Throwing and racket sports
Swimming
Shoulder stability
Force transfer through the upper limb
When the demands placed on the shoulder exceed what the tendon is currently able to tolerate, symptoms can develop.
This is often similar to how tendon pain develops elsewhere in the body — such as Achilles tendinopathy or patellar tendon pain.
Why Does Rotator Cuff Pain Develop?
Research suggests shoulder pain is rarely caused by one single factor.
Common contributing factors include:
Sudden increases in training load
Repetitive overhead activity
Deconditioning or reduced strength
Poor recovery between sessions
Changes in gym volume or intensity
Reduced shoulder blade control
Age-related tendon changes
Prolonged inactivity
Interestingly, posture alone is now thought to play a far smaller role than previously believed. Many people have been told their shoulder pain is simply due to “rounded shoulders” or sitting posture, but evidence supporting posture as the main driver of pain is relatively weak.
Instead, current rehabilitation approaches focus more heavily on improving the shoulder’s overall capacity to tolerate movement and load.
What Symptoms Are Common?
Rotator cuff related shoulder pain commonly presents as:
Pain lifting the arm overhead
Pain during pressing exercises
Discomfort reaching behind the back
Pain lying on the affected side
Weakness during gym exercises
Painful catching or pinching sensations
Reduced confidence using the shoulder
Symptoms that gradually worsen over time
Some people notice symptoms after increasing gym training, while others develop pain following periods of repetitive work or sport.
Does Imaging Always Help?

Scans can sometimes be useful, but research consistently shows that imaging findings do not always correlate well with pain levels.
For example:
Many pain-free adults have rotator cuff tears on MRI
Tendon degeneration is common with age
Structural changes do not always require surgery
Imaging alone cannot explain movement tolerance or strength capacity
This is why a detailed physical assessment is often more valuable than relying purely on scan results.
Physiotherapy assessment focuses on:
Movement quality
Strength
Load tolerance
Functional limitations
Irritability levels
Sport or work demands
What Does Research Support for Treatment?
Exercise-Based Rehabilitation
Exercise remains the most evidence-supported treatment for rotator cuff related shoulder pain.
Research consistently shows that progressive strengthening programmes can:
Reduce pain
Improve shoulder function
Improve tendon capacity
Increase confidence with movement
Reduce recurrence risk
This typically includes:
Rotator cuff strengthening
Shoulder blade control exercises
Gradual loading progressions
Stability and control work
Return-to-sport rehabilitation
Importantly, rehabilitation is usually most effective when exercises are progressed appropriately over time rather than simply relying on passive treatment alone.
Manual Therapy

Hands-on physiotherapy techniques can help reduce pain and improve short-term movement tolerance, particularly when combined with exercise rehabilitation.
Treatment may include:
Joint mobilisation
Soft tissue techniques
Movement retraining
Thoracic mobility work
However, research suggests manual therapy works best as part of a broader rehabilitation plan rather than as a standalone solution.
Load Management
One of the key concepts in modern tendon rehabilitation is load management.
This means temporarily adjusting aggravating activities while gradually rebuilding shoulder capacity.
Complete rest is rarely the answer.
Instead, physiotherapy often focuses on:
Keeping the shoulder active
Modifying painful exercises temporarily
Rebuilding tolerance progressively
Improving recovery strategies
Guiding return to sport or training
Do You Always Need Surgery?
Most cases of rotator cuff related shoulder pain improve successfully with conservative management.
Research comparing surgery to physiotherapy for many shoulder conditions has shown that structured rehabilitation often provides similar long-term outcomes — particularly in non-traumatic cases.
Surgery may still be appropriate in certain situations, such as:
Large traumatic tears
Significant weakness following injury
Failed long-term conservative management
Specific structural pathology
However, many people recover well without needing surgical intervention.
Physiotherapy for Shoulder Pain in Farnborough
At Centre of Gravity Physiotherapy Farnborough, treatment combines evidence-based rehabilitation with detailed individual assessment.
Management is tailored around:
Your symptoms
Training goals
Sport or work demands
Strength deficits
Movement patterns
Recovery capacity
Whether your shoulder pain started in the gym, through sport, manual work, or gradually over time, the aim is always to restore confidence, strength, and long-term shoulder function — not simply provide short-term symptom relief.
If shoulder pain is limiting your training, sleep, work, or everyday activities, physiotherapy can help you understand the problem clearly and build a structured plan towards recovery.

Written By
Harry Liniker BSc MSc MCSP
Lead Physiotherapist and Founder, COG Physiotherapy Farnborough